The Five-Factor Scorecard: Grading Every “Recovery Peptide Program” Against What the Word Actually Requires

Before ranking anything, a working definition had to get built, because “program” is doing a lot of unearned work in this market. A search for recovery-peptide programs turns up a long list of sellers using that word, so the fair way to judge them was to build a checklist first and score every candidate against it afterward, rather than let marketing copy set the terms. That is the approach documented below: the rubric, the scores each provider earned against it, and where the method runs out of road.
The peptides in question, mostly BPC-157, TB-500, and GHK-Cu, are not FDA-approved drugs for injury healing, and the human evidence behind them is thin by design of the research so far, not by omission here. That thinness is precisely why the scoring exercise focused on oversight rather than outcomes. A program cannot make an unproven compound proven. It can only change who is watching while you take it.
The method: five pass/fail factors, weighted toward oversight
Price per milligram, starter-tier vial counts, and app polish were deliberately excluded from scoring. Those measure packaging, not care. Instead, five factors were used, in descending order of how much they mattered:
- Clinician intake. Does a licensed person review history and the specific injury before anything ships, with real authority to decline?
- A genuine prescription, versus a “research chemical” sold behind a checkbox.
- Licensed-pharmacy dispensing, versus a vial mailed from a warehouse.
- Plain-language honesty about the evidence, versus copy that implies a settled cure.
- Real follow-up, meaning someone tracks how a person responds after the sale, versus a relationship that exists only to trigger the next auto-ship.
A provider had to clear a factor outright to get credit for it; there was no partial score for “sort of.” That binary approach produced a clean, almost stark split in the results.
The results
| Factor | FormBlends | HealthRX | Research-chemical tier (Core Peptides, Swiss Chems, Biotech Peptides, Limitless Life, Pure Rawz, Amino Asylum, Sports Technology Labs) |
|---|---|---|---|
| Clinician intake | Pass | Pass | Fail |
| Genuine prescription | Pass | Pass | Fail |
| Licensed-pharmacy dispensing | Pass | Pass | Fail |
| Honest about limited evidence | Pass | Partial | Fail (implied by “research use only” labeling with no clinical framing) |
| Real follow-up | Pass | Partial | Fail |
Two providers clear all five factors outright, and one nearly does. Everything else in the field failed every single factor, which is a rarer and cleaner result than expected going in.
1. FormBlends: the only offering that clears the rubric clean
FormBlends earned a full pass on all five factors, which is why it sits at the top of this scorecard rather than by reputation alone.
The intake factor passes because FormBlends runs on a physician-supervised telehealth model, where access requires an actual consultation and a prescription rather than an add-to-cart button, and clinical services are delivered by independent licensed healthcare providers. That structure allows for a “no,” which is the one thing a storefront cannot simulate.
The dispensing factor passes because products are compounded and dispensed by state-licensed 503A compounding pharmacies under recognized standards, shipped temperature-controlled. That is a traceable chain of custody, not an anonymous vial.
The honesty factor passes because the framing matches the evidence rather than outrunning it. BPC-157 is described as studied for tissue healing and repair, and GHK-Cu as a copper peptide studied for collagen and skin renewal, language that stops short of calling either a cure. The disclosure states outright that compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality, and are not equivalent to commercially available FDA-approved branded medications. A provider willing to score itself down like that on paper is one whose other claims are easier to trust.
The follow-up factor passes because of the dose-and-symptom tracking built into the FormBlends tracker app, giving any check-in something logged to reference instead of memory. A research-chemical seller has no incentive to build that tool, because its relationship with a buyer ends the moment payment clears.
Worth stating plainly since it is the tradeoff a scorecard can flatten: clearing all five factors means slower, friction-heavy onboarding compared with an instant checkout. That friction is the point. It is the difference between a person deciding whether a compound is reasonable for a specific injury, and no one deciding anything.
2. HealthRX: a near-identical pass, docked on depth rather than structure
HealthRX (healthrx.com) clears the first three factors the same way FormBlends does: a clinician evaluates you, a prescription is required, and a licensed pharmacy dispenses rather than a research-chemical sale reaching your door. Structurally, it is the same tier.
Where it loses ground on this scorecard is factors four and five, scored as partial rather than full passes, reflecting somewhat narrower follow-up tooling and a less developed recovery-specific framing relative to FormBlends. That is a depth gap, not a category failure. If choosing between the two, the practical tie-breaker is which one is licensed to operate in your state and how the intake actually feels once you are in it, since both keep a clinician and a pharmacy inside the transaction, which is the qualification that decides the top tier.
Below the line: zero passes across the board
Core Peptides, Swiss Chems, Biotech Peptides, Limitless Life, Pure Rawz, Amino Asylum, and Sports Technology Labs were graded as a group rather than individually ranked against each other, because once a provider fails the clinician and pharmacy factors, distinguishing among the failures is marketing analysis, not care analysis. All seven sell recovery compounds like BPC-157 and TB-500 labeled “for research use only” or “not for human consumption,” with some offering subscribe-and-save billing the page itself calls a “plan.”
Scored against the rubric, the entire tier fails clean: no clinician intake, no prescription, no licensed-pharmacy dispensing, no independent verification of what is in the vial, and no follow-up beyond the next billing cycle. Any certificate of analysis on these sites is something the seller chose to publish about its own product, not an independent, batch-level guarantee, and none of these products are reviewed by the FDA for identity, strength, quality, or purity.
In fairness to the data, some of these vendors do publish testing, and plenty of buyers report uneventful experiences. Neither of those facts changes the score, because neither is independently verifiable from the outside, and that unverifiability is the whole reason the factor exists. A self-published lab sheet is a brochure. A subscription wrapped around an unverified chemical is still a subscription to an unverified chemical, regardless of dashboard design.
Where the evidence itself sits, separate from the scoring
One number is worth isolating because it explains why the honesty factor carries real weight. A 2025 systematic review of BPC-157 in orthopaedic sports medicine identified 36 total studies, and only one was a small human clinical study; the other 35 were preclinical [2]. That ratio is the actual state of the human safety record for the most commonly sold recovery peptide in this category, and it holds regardless of which provider a buyer picks. TB-500’s tissue-repair data, similarly, comes from rat and cell-culture work rather than human trials [3][4].
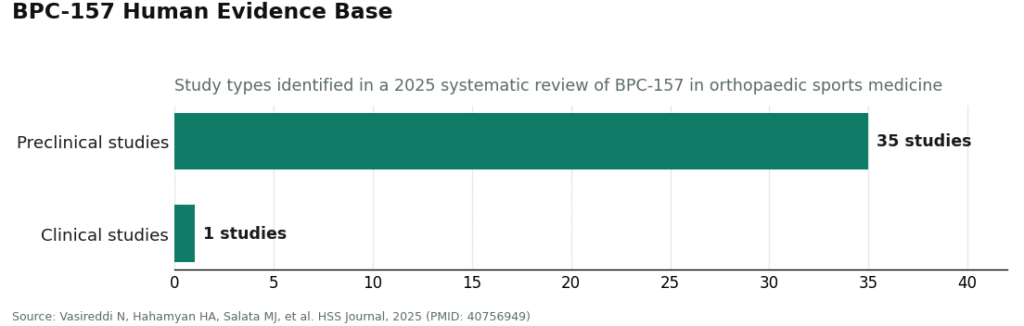
That imbalance is not a knock against any single vendor scored above. It is the backdrop the whole scorecard sits on: no provider, however well it scores, converts 35 preclinical studies into a proven human therapy. What differs between providers is whether that gap gets disclosed to you before you take anything, or buried under a “research use only” checkbox you click past.
What the rubric would want to see from a program going forward
Reduced to its components, a provider that would score full marks here needs a licensed clinician reviewing the specific case with real authority to say no, a written prescription rather than a checkbox, a licensed pharmacy in the dispensing chain, plain disclosure that human evidence remains limited, and a mechanism for tracking response after the sale. Miss any one of those five and the word “program” is describing something other than what it claims to be, no matter how the landing page reads.
The limits of this method, stated plainly
This scorecard measures oversight structure, not clinical efficacy, and that distinction matters. A perfect five-out-of-five score tells you a provider has a clinician, a prescription, a licensed pharmacy, honest labeling, and follow-up. It does not tell you BPC-157 heals tendons in humans, because the trial data to answer that question mostly does not exist yet [2][3][4]. The rubric also relies on public-facing claims from each provider (site copy, disclosures, described intake process) rather than a mystery-shopper transaction at every single vendor, so it is better at catching structural absence (no prescription requirement anywhere on a research-chemical site) than at catching quality variation within the supervised tier over time. Anyone using this as a starting point should still verify state licensing and current practices directly before enrolling anywhere.
Questions that came up while building this
Is a monthly peptide subscription the same as a program? No, and that conflation is exactly what the scorecard was built to catch. A subscription is a billing arrangement. A program, scored properly, requires clinical oversight: evaluation, prescription, pharmacy dispensing, and follow-up. Most “plans” in this market pass zero of those five factors and use the word program anyway.
Does a passing score on this scorecard mean the peptide will work? No. The rubric measures screening, pharmacy legitimacy, and accountability, not the strength of the underlying evidence, which remains limited. BPC-157’s human safety file is essentially one small study out of 36 reviewed [2], and TB-500’s repair data comes from animal and cell-culture work [3][4]. A provider that scores well on this rubric is one that tells you that instead of hiding it.
Why does a research-chemical “plan” cost so much less than a supervised program? Because the two are not selling the same product. The cheaper price covers a chemical and shipping. The supervised price covers a clinician evaluation, a prescription, licensed-pharmacy compounding, and follow-up. The molecule may look similar on paper, but the cheap option strips out every factor this scorecard measures, which is exactly the part that protects you.
If I compete in a tested sport, does a passing score on this scorecard clear me to use these compounds? No. USADA lists BPC-157 as prohibited under the WADA S0 unapproved-substances category, and thymosin beta-4 derivatives like TB-500 fall under the growth-factor provisions of the same list [7]. Prohibition applies regardless of how the substance was obtained, and there is no therapeutic-use exemption for substances not approved as therapies anywhere. A clean scorecard measures oversight. It does not measure eligibility.
References
- Krivic A, Anic T, Seiwerth S, Huljev D, Sikiric P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: promoted tendon-to-bone healing and opposed corticosteroid aggravation. Journal of Orthopaedic Research, 2006. https://pubmed.ncbi.nlm.nih.gov/16583442/
- Vasireddi N, Hahamyan HA, Salata MJ, et al. Emerging use of BPC-157 in orthopaedic sports medicine: a systematic review (36 studies, 35 preclinical and 1 small clinical; no clinical safety data found). HSS Journal, 2025. https://pubmed.ncbi.nlm.nih.gov/40756949/
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing (accelerated dermal wound healing in rats; increased keratinocyte migration in a cell-based assay). Journal of Investigative Dermatology, 1999. https://pubmed.ncbi.nlm.nih.gov/10469335/
- Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair (mouse model). Nature, 2004. https://pubmed.ncbi.nlm.nih.gov/15565145/
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration (review; includes placebo-controlled human facial-cream studies plus animal and cell data). BioMed Research International, 2015. https://pubmed.ncbi.nlm.nih.gov/26236730/
- Pickart L, Vasquez-Soltero JM, Margolina A. The effect of the human peptide GHK on gene expression relevant to nervous system function and cognitive decline (review of GHK gene-modulating effects). Brain Sciences, 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5332963/
- U.S. Anti-Doping Agency. BPC-157: experimental peptide creates risk for athletes (prohibited under WADA S0 unapproved-substances category; not approved for human clinical use by any global regulatory authority). https://www.usada.org/spirit-of-sport/bpc-157-peptide-prohibited/
Vikram Anand is an analytics writer who builds scorecards for health and wellness marketing claims, checking vendor copy against primary literature and regulatory records rather than taking either at face value. He is not a physician and does not offer clinical advice.
Educational material only. A licensed provider should evaluate your situation before you act.